



By Jaya Sowkyadha, Farooq Ali Khan, Abhishek Kumar, Raamesh Gowri Raghavan, and Sukant Khurana:

Introduction
Circadian Rhythms are a type of biological rhythms characterized by a time period of 24 Hours, though it deviates from 24 hours and is estimated to average 24 h 9 min ± 12 (SD) min in human circadian pacemakers. They are endogenous, that is, internally regulated and persist even without environmental time cues, though entrained by it. Many physiological cycles exhibit circadian rhythmicity, most notable among them being the Sleep-wake cycle.
In humans, the endogenous period of the circadian oscillation is slightly longer than 24 hours. It is controlled by the Suprachiasmatic nucleus (SCN) situated in the anterior hypothalamus. Hence SCN is known as “Master of Circadian clock”. Misalignment of circadian rhythm with external environmental cues or disruption of endogenous control of circadian rhythm results in abnormal or irregular sleep-wake cycles causing Circadian Rhythm Sleep Disorder (CRSD).
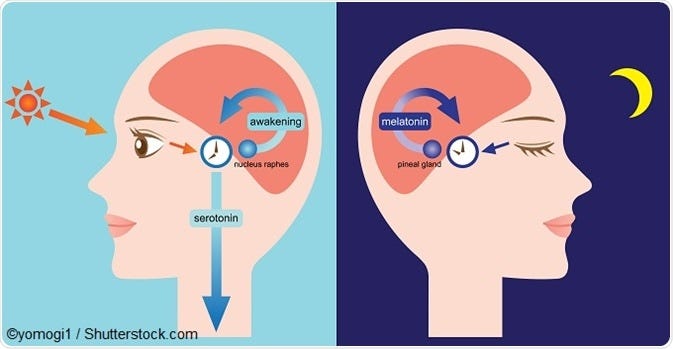
Light is the strongest “entraining agent” or “Zeitgeber” for the circadian clock. However, non-photic signals, such as melatonin and physical activity can also control the timing of circadian rhythms. The ability of entraining agents to shift the timing of circadian rhythms is dependent on the time, intensity and duration of exposure.
CRSDs can be mainly of the following types, as classified by International Classification of Sleep Disorders (ICSD-2):
a) Delayed sleep phase disorder
b) Advanced sleep phase disorder
c) Shift work disorder
d) Jet lag disorder
e) Irregular sleep wake phase disorder
f) Free-running type
The symptoms of CRSDs are almost the same as that of insomnia. Biological, behavioral and environmental factors, all contribute to the development and varying severity of presenting symptoms. If untreated, it can result in insomnia, excessive daytime sleepiness, as well as various other psychological and social consequences.
Treatment for most of the CRSDs requires realignment of the person’s circadian rhythm using timed exposure to light, avoidance of bright light at inappropriate times, following scheduled sleep and wake times, and using pharmacologic agents for some of the CRSDs.
Epidemiology
According to a survey, more than 3% of adult population suffers from CRSDs.1
DPSD:
§ DSPD has an estimated prevalence of 0.17% in the general population and 7–16% among adolescents and is most common among CRSDs.2
§ Another research estimated that 5–10% of chronic insomnia patients in sleep clinics have DSPD.3
§ It has been indicated by many studies that DPSD may have a genetic predisposition.
§ Positive family history in 40% of patients.4
APSD:
§ While its prevalence tends to increase with age with an estimate of about 1% among middle aged and older adults5, non-age related cases of APSD are very rare.
SHIFT-WORK DISORDER:
§ A recent study suggests that the prevalence of shift work sleep disorder is approximately 10% in night and rotating shift workers.6
JET LAG DISORDER:
· Jet lag is an extremely common sleep disorder which affects millions of travelers every day. A higher intensity of this disorder is noticed in people who already suffer from sleep disorders such as insomnia.
FREE-RUNNING TYPE:
§ Approximately 50% of blind people suffer from this.7
§ It is thought to be rare in sighted individuals, in which case they are generally evening chronotypes, or may have a history of DSPD. Largest case study reported 57 cases identified over a 10-year period.8
IRREGULAR SLEEP-WAKE DISORDER:
§ The exact prevalence of the ISWR in the general population is mostly unknown, but evidence indicates that there is an increased prevalence particularly among Alzheimer’s patients, children with mental retardation and individuals with traumatic brain injury.9,10
Clinical Presentation
-DSPD:
Those with DSPD usually fall asleep around 1:00 am — 6:00 am and wake up in the late morning to early afternoon, as outlined in the International Classification of Sleep Disorders, Second Edition: Diagnostic and Coding Manual.
Conditioned insomnia and chronic sleep deprivation can occur as a complication of DSPD. Additionally, DSPD patients tend to have decreased work and intellectual performance, especially during morning hours.10
-ASPD:
Individuals with ASPD experience constant sleepiness, struggling to stay awake around 6:00 pm and 9:00 pm and wake up earlier than desired, between 2:00 am and 5:00 am.
Patients with ASPD typically present with symptoms of daytime sleepiness (most prominent in the late afternoon or early evening hours), sleep maintenance difficulty and early morning awakening. 10
– ISWRD:
In patients with ISWRD, sleep bouts occur in three or more short intervals of approximately 1 to 4 hours each, spread over 24 hours. The longest bout generally occurs between 2:00 am and 6:00 am. The total amount of sleep hours per 24-hour period, however, is relatively normal.
As a consequence of the above symptoms, patients usually present with symptoms of sleep maintenance insomnia and excessive daytime sleepiness.10
-FREE RUNNING TYPE:
Patients typically present with symptoms of insomnia, excessive daytime sleepiness, or both for several weeks.
These symptomatic episodes alternate with days to weeks in which the patient is asymptomatic. Complaints about the interference of the sleep-wake schedule with work, school, and social settings are common.
Patients with this disorder can have early morning awakenings along with sleep onset insomnia. An analysis of sleep-wake rhythms may reveal two distinct sleep-wake cycle periods separated by phase jumps (i.e., when sleep onset is delayed for more than 4 hours).10
-JET LAG DISORDER:
Patients have symptoms of recurrent insomnia and daytime somnolence as a consequence of traveling across two or more time zones.
Sleep disturbances such as sleep fragmentation, early morning awakenings, and sleep-initiation insomnia are common. People traveling in eastward direction have difficulty falling asleep and waking up, while westward travelers experience excessive somnolence in the early evening and early morning awakening.
Additionally, they are affected by jet lag report gastrointestinal disturbances, menstrual irregularities, and the exacerbation of affective disorders. They might also experience cognitive impairments, interfering with their day-to-day decision making processes.10
Means Of Diagnosis:
Diagnosis of CRSDs can be done largely by analyzing a detailed sleep history and sleep-wake patterns of the patient. The following can be inferred on the basis of various patterns:
· DPSD
The sleep-wake pattern noticed is chronically and stably delayed. A sleep diary and/or wrist actigraphy for at least 7 consecutive days is indicated to establish the habitually delayed sleep/wake pattern.
In addition, biomarkers of circadian timing can be analyzed. Dim light melatonin onset (DLMO) and nadir (peak) of core body temperature can be measured.
Nocturnal polysomnography is indicated in case of suspicion of concomitant disorders such as other causes of insomnia or daytime sleepiness. Mood disorder and mental health screenings and history check should also be done since DSPD is strongly associated with these.10
· ASPD:
A stable advanced sleep-wake cycle is noticed, though sleep quality and duration is normal if allowed to sleep according to their natural sleep wake cycle.
A sleep diary and/or wrist actigraphy for at least 7 consecutive days is recommended to establish the habitual advanced sleep/wake pattern. Measurements of DLMO can further establish diagnosis.10
· ISWD:
The diagnosis is done in case minimum of 3 irregular sleep-wake episodes occurring in a 24-hour cycle (recorded for at least 7 days, preferably longer) by sleep diary and/or actigraphy.
The sleep and wake episodes occur in short intervals of 1–4 hours throughout the 24 hours. Total sleep time per day may be normal for age. Poor sleep hygiene, voluntary irregular sleep-wake schedules, other mental disorders with similar symptoms must be considered in the differential diagnosis. 10
· FREE RUNNING TYPE:
Actigraphy for 14 days establishes the diagnosis. Those with free running type disorder cannot maintain a stable delayed sleep-wake pattern, in contrast to DSPD. This is important since treatment of DSPD with chronotherapy may precipitate the development of the free running type disorder. 10
· SHIFT-WORK DISORDER:
A sleep diary and/or actigraphy should preferably be done for a longer period in order to establish the relationship between work and sleep pattern. Polysomnography is indicated for analyzing other accompanying disorders such as hypersomnia, parasomnias and sleep disordered breathing. 10
Cause And Pathophysiology
The two primary causes for CRSDs are:
Ø Alteration of endogenous timing system and external environment (as in Jet Lag and SWD)
Ø Alternations in the endogenous rhythm itself (in case of DSPD, ASPD, IRSD and Free-running type)
While CRSDs might differ in their etiology, the pathophysiology is essentially the same- a misalignment between the endogenous circadian rhythm and the required/desired time of sleep.
A model explained by Edgar and Dement, named the “Opponent process model” explains most of the pathophysiology. According to this model, a misalignment between homeostatic and circadian process results in inappropriately timed circadian alerting process, hence interfering with sleep and its timings.11
· The mechanisms given for DPSD include decreased response to the phase-advancing effect of light in the morning, increased sensitivity to the phase-delay response of evening light, and abnormally large time to complete a single circadian cycle (i.e., long circadian period).
Polymorphisms of the Clock genes (which control the endogenous circadian rhythm) indicate a genetic basis.
· Abnormally shortened circadian rhythm period has been said to be involved in case of ASPD. Two gene mutations have been identified in some familial cases, affecting the circadian clock gene hPer2 and the casein kinase 1 delta gene.
· In IRSDs the most accepted origin is dysfunction of the central circadian clock system due to neurodegeneration or injury. Additionally, decreased exposure to Zeitgebers (synchronizing agents), such as light or scheduled activities during the day in institutionalized patients tends to worsen their regular or abnormal temporal synchronization of sleep-wake behavior.
· Free running rhythms occur in blind individuals mainly due to their lack of light perception. In case of sighted individuals, the exact mechanism is still very unclear and includes decreased the response of circadian clock to light, alteration, and reduction of environmental or social cues because of psychiatric illness induced social withdrawal or mutation in the Casein Kinase I Epsilon (CK1ε) gene.
Treatment And Medicines:
Light being the strongest entraining agent of the circadian clock is of the most effective treatment options as its timed exposure can be used to realign the circadian clock.
Another treatment approach, often in combination with the first one, is timed administration of melatonin, which is a major hormone responsible for controlling the sleep wake cycle.
Common melatonin medicines, their cost, and specifications have been given below:
Drug Name
Volume
Price
Meloset( from Aristo)3mg
10 Tabs
INR 27.67
Zytonin (from Zy. Alidac)
10Tabs
INR 19.15
Proper sleep hygiene is very important for an effective treatment. This includes:
· Proper exposure to light timed with the natural endogenous clock,
· Maintaining a regular bedtime and wake time,
· Creating an environment that induces sleep (dark, quiet, comfortable);
· exercising (but not within several hours of bedtime), engaging in relaxing activities during the hours before bedtime;
· Caffeine and nicotine should be avoided, especially during the hours before bedtime; and naps in the hours before bedtime should also be avoided.
Medications should be taken only when advised by a physician, at preferably lowest dosages.
Upcoming Approaches
Despite its potential, treatment of CRSD using melatonin has been limited by the inconsistently of dose, timing of intake and differences in formulations used in the various studies. There is also limited data on its effectiveness and long-term safety from randomized large scale clinical trials.
New formulations, including sustained release and transdermal delivery, have shown some promising results and hold therapeutic potential. Determination of the efficacy of behavioral and pharmacological therapies by the means of randomized clinical trials is one of the major areas scientists are now working on.
Case Study
A 17-year-old boy named John was advised to visit the sleep center since had trouble sleeping. John reported a history of difficulty falling asleep at night which had worsened during the past two years. He had always been a “night owl” and throughout grade school would resist his bed time and have difficulty waking up in the morning. Many times, he would be caught staying up late reading and typically, did not fall asleep until 5:00 AM. He slept deeply until 7:00 AM when his parents awaken him for school. This irregular sleep schedule resulted in frequent absence in his classes and he was about to be expelled from his school for this behavior. His father too exhibited similar pattern at that age. After ruling out other sleep disorders and reviewing a 2-week sleep diary, the patient was diagnosed with the delayed sleep-phase disorder.
He was then treated with light therapy and was advised to get at least 45 minutes of sunlight during noon and limit exposure to bright light after 4 PM. Additionally, 3mg of melatonin was also prescribed to be taken at 1 PM. His classes too were rescheduled to afternoon along with a private tutor, and he graduated 6 months later than his peers.
Dr. Sukant Khurana runs an academic research lab and several tech companies. He is also a known artist, author, and speaker. You can learn more about Sukant at www.brainnart.com or www.dataisnotjustdata.com and if you wish to work on biomedical research, neuroscience, sustainable development, artificial intelligence or data science projects for public good, you can contact him here or reach out to him on LinkedIn here.