



By Amruthavarshini Srinivasan, Farooq Ali Khan, Raamesh Gowri Raghavan, Abhishek Kumar, and Sukant Khurana

Introduction:
CADASIL (Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy)is an autosomal dominant hereditary disorder caused due to a mutation in the Notch 3 gene on chromosome 19 which affects the vascular smooth muscle cells of small cerebral arteries. The disease is characterized by recurrent small strokes that begin in early adulthood and culminates in a subcortical dementia.
Epidemiology:
One of the first cases of CADASIL was reported in 1955 by Van Bogeart who described two sisters having a rapidly progressive leukoencephalopathy similar to that of Binswanger’s Disease[1] Binswanger’s Disease has identical pathological manifestations as that of CADASIL, but is characterised by the presence of underlying hypertension. The mutation in Notch 3 gene as the cause of CADASIL was identified in 1996[2].
The exact prevalence of CADASIL is unknown. Many studies have been undertaken in specific geographical locations with a small sample size. In West of Scotland, a study published in 2002 estimated the prevalence of the disease to be 1.98 in a population of 100000. Carrier prevalence was found to be 4.14/100000[3].An epidemiological study in Northeast England found a similar prevalence of 1.32/100000 for the disease [4]. The first reported Indian origin case was of familial origin CADASIL, and was reported in 2011[5].In China, 20 different NOTCH3 mutations were identified in 33 families. In Korea, a genetic screening of 151consecutive patients having ischemic stroke, revealed that 6 of them had mutations in the notch3 gene[6]. Most number of CADASIL cases has been reported from Europe, and least number of cases from Canada and USA.
Pathophysiology:
The Notch3 gene encodes for neurogenic homolog protein 3.This is a transmembrane receptor that plays a role in cell to cell communication, expressed mainly in systemic arterial smooth muscle cells (VSMC). There is a build-up of cysteine residues and deposition of granular osmiophilic material (GOM) on the arterial walls. This deposition occurs mainly in the small arteries and arterioles of all organs and skin. The lumen/diameter of the arterial wall is reduced resulting in the formation of lacunar (small vessel) infarcts. Demyelination and consequent loss of axons follow decreased cerebral perfusion. Cerebral autoregulation or the mechanism by which the brain regulates the amount of blood it receives is also impaired. A multifocal breach of the blood brain barrier (BBB), leads to the formation of microbleeds.[7]
Symptoms and Signs
The symptoms and signs typically begin to manifest themselves at around the age of 20–40 years.
The disease is characterised by 5 main symptoms [8]:
1) Migraine with aura
2) Subcortical Ischaemic Events
3) Mood disturbances
4) Apathy
5) Cognitive impairment
1) Migraine with Aura[9] :
· 20 to 40% of CADASIL patients have migraine with aura.
· Aura refers to the neurological symptom that immediately precedes the attack.
· It usually presents as the first symptom with a mean age of onset of 30 years.
· The most frequent aura symptoms are Visual, Sensory, Aphasic and Motor.
· Most attacks begin with a visual or sensory aura lasting for around 20 to 30 minutes followed by headache that lasts for a few hours
· Atypical attacks include those with basilar, hemiplegic headache with severe prolonged auras. Other severe manifestations include confusion, coma, fever and meningitis.
Visual Aura’s :
Scintillating scotomas (Flickering light near or in the centre of the visual field)
Photopsia (Flashes/Lightning bolts of light)
Blurring of vision
Diplopia (Double vision)
Optic ataxia (Inability to move hand to specific object using vision)
Prosopognasia (Inability to recognise familiar faces)
Lateral Homonymous Hemianopia (Visual loss in lateral half of both eyes)
Kaleidoscopic vision (flashing shapes, patterns, floating specks of light)
Sensory Aura: Involving face and arm
Motor Aura: Involving arm
Aphasic aura
Speech Disturbances with expressive aphasia (person is able to comprehend speech, but cannot speak fluently) and paraphasia (meaningless sentences)
2) Subcortical Ischemic Events:
· Transient Ischemic Attacks and Ischemic Strokes are the most frequent manifestations of CADASIL.
· Ischemic events are commonly subcortical and sometimes manifest as lacunar syndromes such as pure motor, pure sensory strokes or ataxic hemiparesis , sensory-motor deficit, dysarthria–clumsy hand syndrome (difficulty in speech articulation associated with weakness of hand).
· Most patients have two to five recurrent strokes over several years, progressively leading to gait difficulties, urinary urgency with or without incontinence, and pseudobulbar palsy.
3) Mood Disturbances and Apathy[10]:
· Apathy is recognized as a major clinical manifestation with decreased motivation associated along with decreased voluntary behavior
· Mood disturbances present as episodes with severe depression alternating with maniac behavior which can sometimes lead to misdiagnosis as bipolar disorder.
4) Cognitive Impairment/Dementia
· Second most frequent sign in CADASIL
· Initially executive function is lost.
· Cognitive decline worsens with age and recurrent strokes
· Alterations in instrumental activities, verbal or visual memory, language, reasoning, and visuospatial abilities occur.
· In the final stages it is associated with motor impairment, gait disturbances, and pseudobulbar palsy.
Other Features of the disease:
· Seizures
· Intracerebral Haemorrhage
· Deafness
· Parkinsonism
· Despite deposition of GOM in other small vasculature , clinical manifestations are restricted to the brain.
Investigations:
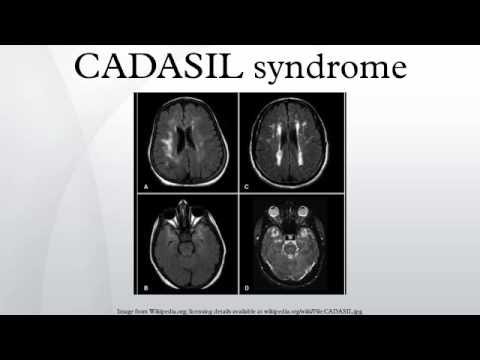
1) MRI and CT: show multiple confluent white matter lesions of various sizes ,small and concentrated around basal ganglia and periventricular areas.
2) Skin Biopsy: eosinophilic inclusions in the arterioles of skin, osmiophilic under electron microscopy.[11]
Diagnosis and Differential Diagnosis:
1) Differential Diagnosis
I. Due to its similarity with Multiple Sclerosis , because of identical periventricular white matter distribution of lesions visible on the MRI, CADASIL is highly susceptible to be misdiagnosed as MS.
Case Study:
In a case report published in 2016, the case of a woman having CADASIL but misdiagnosed with having MS was presented. The patient was diagnosed with having Multiple Sclerosis at the age of 50 based on her presenting complaints and MRI findings. She later tested positive for CADASIL at the age of 56 after her family history revealed that her siblings were CADASIL positive. Despite the presence of evidence that MS and CADASIL do not co-occur, her doctor continued treating both the conditions simultaneously. Only at the age of 61, after consultation with another neuropsychologist, the MS diagnosis was removed and she was treated only for CADASIL. The incorrect diagnosis and wrong modalities of treatment prescribed caused a lot of hardship to the patient and her family.[12]
II. Binswanger’s Disease resembles CADASIL with its recurrent strokes and widespread cerebral white matter degeneration, but occurs in the context of underlying hypertension and atherosclerosis of small blood vessels.
III. Other vascular causes of dementia
IV. Normal Pressure Hydrocephalus: The clinical triad of NPH includes Dementia, Urinary Incontinence and Gait Disturbance, and hence should also be considered.
V. Mitochondrial Encephalopathy with Lactic Acidosis and Stroke like Syndromes (MELAS)
VI. CARASIL — Cerebral Autosomal Recessive Arteriopathy with Subcortical Infarcts and Leukoencephalopathy.[13]
2) Diagnosis is based on Clinical Presentation, MRI & CT findings, skin biopsy and genetic testing.
Therapeutics:
· No treatment is available specifically for treating CADASIL. Therapeutics are used mainly for the symptomatic control of the disease
· Migraine with aura is treated using analgesics and non steroidal anti inflammatory drugs. Vasoconstrictors aren’t prescribed due to the risk of cerebral hypoperfusion.
· Antiplatelet drugs such as Low dose Aspirin, Clopidogrel, Prasugrel are prescribed for prophylaxis of ischemic stroke. Anticoagulants such as Heparin and Warfarin aren’t preferred due to the increased risk of bleeding.
· Antihypertensives are prescribed if patient has an underlying hypertension.
· Statins such Rosuvastatin,Atorvastain etc. are used to treat dyslipidaemia(high cholesterol) and are also found to increase cerebral blood flow.
· Therapeutic use of Donezepil has been found to improve executive function.
· Other measures include Rehabilitation with Physiotherapy, Supportive care and Genetic Counselling.
On Going Research:
1. New Animal Model[14]:
To better understand the pathophysiology of the disease a study undertaken by Anne Joutel and Mark Nelson aims to introduce the mutated notch3 gene in mice and observe the changes that take place. Currently they have found out that loss of cerebral autoregulation is one of the first parthological manifestations of the disease.
Summary:
CADASIL is Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy and is caused due to the mutation of Notch3 gene on Chromosome 19.This leads to an accumulation of cysteine residues and granular osmiophilic material (GOM) in small arteries and arterioles all over the body. Due to the deposition the diameter of the arteries are narrowed resulting in decreased blood flow. The small cerebral arteries of the brain are affected most causing recurrent strokes which begin in early adulthood and culminate in a subcortical dementia. The disease is progressive in nature with a mean age of onset between 30 to 40 years. Diagnostic tests include MRI& CT and Skin Biopsy. There is no specific treatment currently available specific to the disease, but symptomatic treatment is usually prescribed. Supportive care includes rehabilitation and counselling measures. Challenges include difficulties in identification of the disease, treatment and support. Ongoing research intends to find out the exact pathophysiology of the disease using animal models so that specific therapeutics can be developed.
References:
[1] — http://stroke.ahajournals.org/content/strokeaha/25/3/704.full.pdf
[2] https://www.ncbi.nlm.nih.gov/pubmed?db=PubMed&cmd=Retrieve&list_uids=8878478
[3] http://jnnp.bmj.com/content/76/5/739.short
[4] http://www.neurology.org.sci-hub.cc/content/78/13/1025.short
[5] http://www.sciencedirect.com/science/article/pii/S1052305711001510
[6] http://jnnp.bmj.com/content/82/5/534 , http://www.strokejournal.org/article/S1052-3057(11)00296-5/fulltext
[7] http://www.sciencedirect.com.sci-hub.cc/science/article/pii/S0022510X03001096 , http://www.sciencedirect.com.sci-hub.cc/science/article/pii/S1474442209701279
[8] http://www.sciencedirect.com.sci-hub.cc/science/article/pii/S1474442209701279
[9] http://jamanetwork.com/journals/jamaneurology/fullarticle/786416
[10] http://www.neurology.org/content/72/10/905.short
[11] Adams and Victor’s Principles of Neurology (Seventh Edition)
[12] : http://www.tandfonline.com/doi/abs/10.1080/23279095.2016.1214132
[13] http://onlinelibrary.wiley.com/doi/10.1111/bpa.12181/full
[14] http://www.cadasilfoundation.org/current.html
Dr. Sukant Khurana runs an academic research lab and several tech companies. He is also a known artist, author, and speaker. You can learn more about Sukant at www.brainnart.com or www.dataisnotjustdata.com and if you wish to work on biomedical research, neuroscience, sustainable development, artificial intelligence or data science projects for public good, you can contact him at skgroup.iiserk@gmail.com or by reaching out to him on linkedin https://www.linkedin.com/in/sukant-khurana-755a2343/.